
Blog Post
Intelligence for the decisions that matter most
David West
08 Jun 2026
Geoffrey Hinton, Nobel laureate and “Godfather of AI,” said in 2016 we should stop training radiologists. Ten years later, hiring demand is at a record high.
I’ve been building pathology AI for over a decade. Whenever I tell someone what I do, the reaction is some version of Hinton’s prediction: “Ah, so you’re replacing pathologists?” It’s a question that misreads what’s actually happening to the discipline, and what’s about to happen.
The narrative on AI’s impact on white-collar work has, in my time in the field, gone from sci-fi, to clickbait, to zeitgeist. Medical diagnostics attracts an outsized share of the attention – high-expertise work, heavy on pattern recognition, in a life-and-death application; it makes for a good story.
Beyond what any editorialized take captures, though, I’m seeing this in my own work and how my company is run. AI progress has floored me. It’s been nothing short of transformational for what our AI R&D can do.
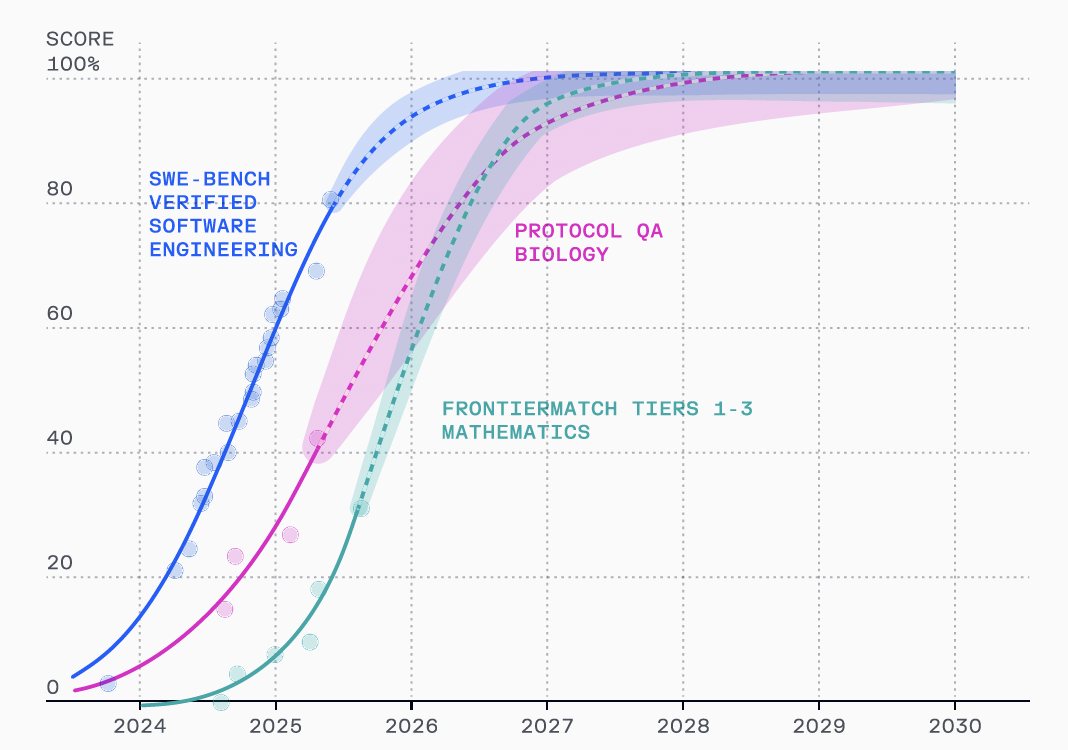
In the past year, AI models reached human-level performance across vision, language, and reasoning (1). They’re on track to hit similar benchmarks in advanced biology and mathematics by 2030 (2).
Part of the allure – or fear or anxiety – is that we have limited visibility into how these developments will play out for humans. Existing economic theories offer some frameworks for how we think about this. Economic optimists (of which I am one) cite Jevons paradox: as cost per task collapses, demand increases. If this holds true, we’re heading to a world of great abundance (great medical abundance in our case).
Early evidence suggests we’re watching Jevons’ predictions play out in real time. 2026 models are already more capable of writing code than most human software developers; agentic coding tools (e.g. Claude Code) are used at every top tech company to write, in many cases, ~90% of new code. Companies, like the one I run, are hiring more software engineers against this backdrop.
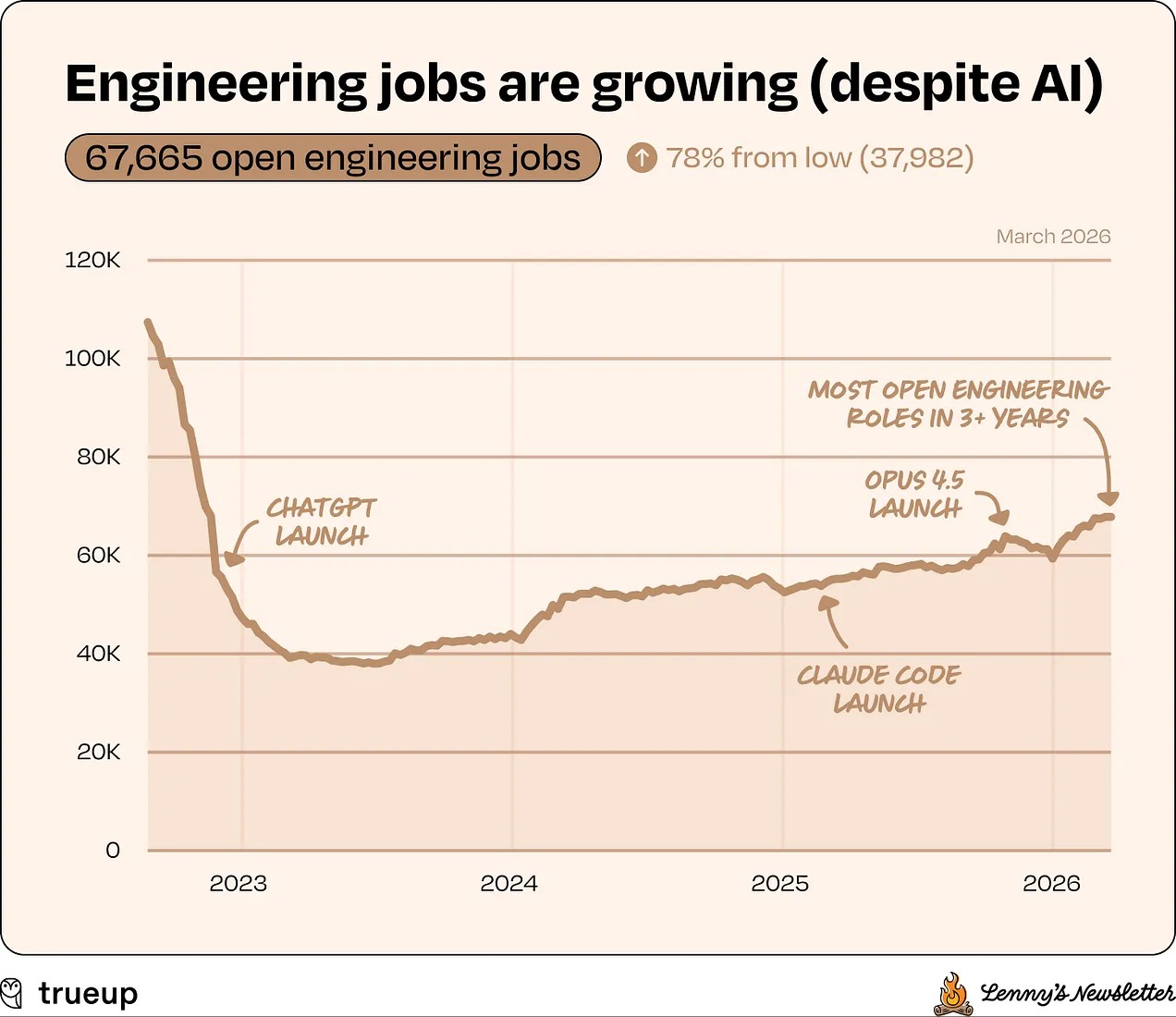
Source: TrueUp, via Lenny’s Newsletter (2026)
In medical diagnostics, AI has been well adopted in radiology since Hinton’s prediction, but Jevons paradox seems to be holding true, at least for now.
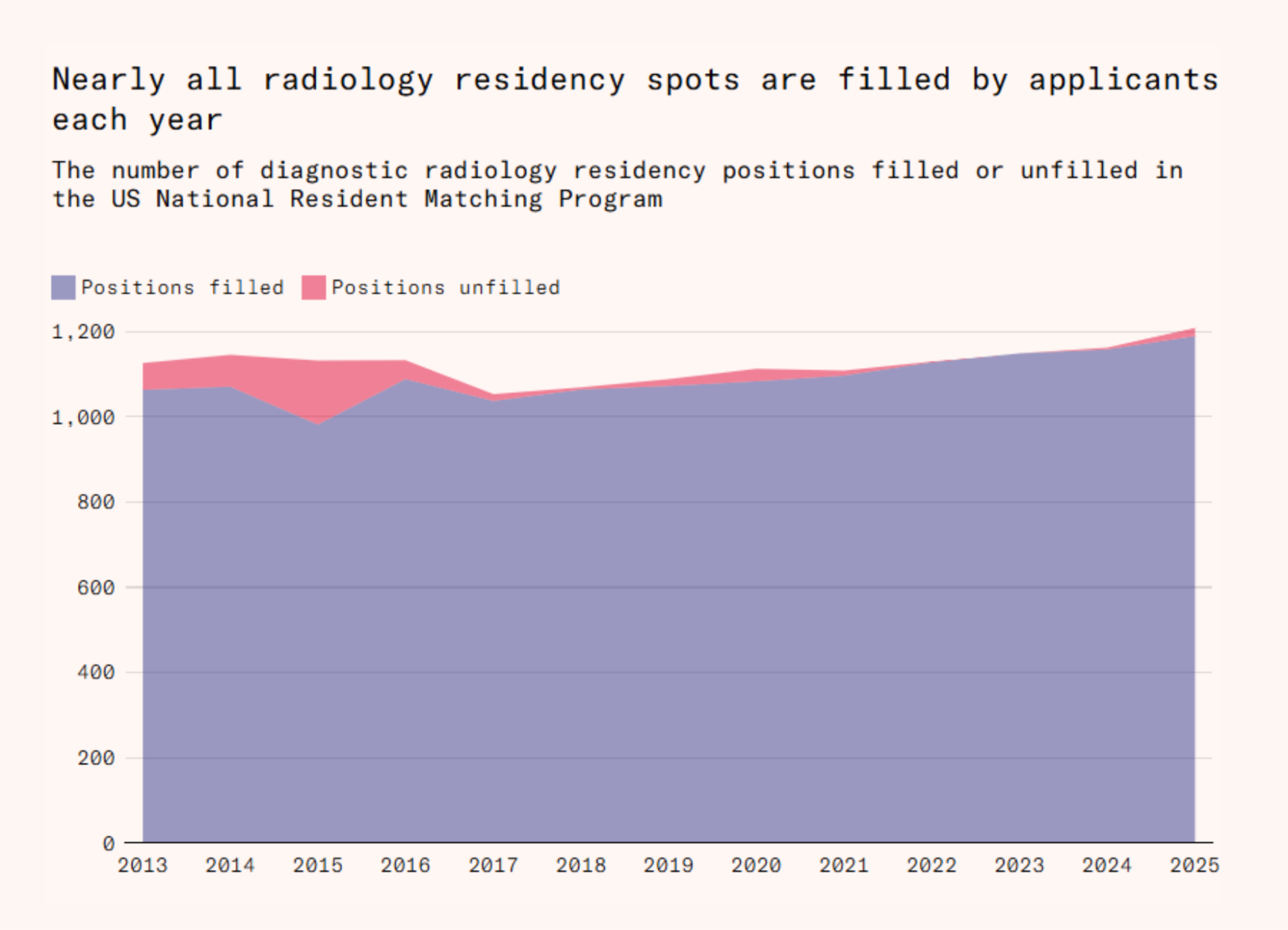
Source: Deena Mousa, “The algorithm will see you now,” Works in Progress (2025); NRMP data
Of note, this pattern is still early and shouldn’t be overinterpreted. Agentic coding adoption has not proliferated beyond top engineers and tech companies. Radiology demand is driven by many factors (rising imaging volume, workforce constraints, and healthcare economics). All of this makes it hard to isolate any causal impact from AI.
And any intellectually honest assessment should admit that no precedent exists for a world in which machines outperform all humans in all cognitive work. Does economic theory hold true past the singularity? What does medicine look like when we have “a country of geniuses in a data center,” as Anthropic CEO Dario Amodei predicts?
How does this play out in pathology? Two visions
Further pontification on the economics or philosophy of AI is better left to the pub. The reality is that AI progress is accelerating. Much of the world is moving through the 5-stages-of-AI-grief (starting with denial). Software engineers had to move through all stages violently, and if Reddit threads count for anything, our community in pathology shares those fears. From Dr. Luis Cano on his Substack:
When the discourse centers on replacement, the professional is no longer competing with an algorithm. They are competing with the idea of their own irrelevance. And that battle is not fought in the lab. It is fought in identity.
Unlike software engineering, pathology does have a window – probably ~2 years – to manage this transition well. Beyond that, there are two divergent scenarios:
Scenario A: pathology shifts further from the center of clinical decision-making, and labs are relegated to a back-end service.
Scenario B: more diagnostic focus and clinical responsibility in the hands of experts, higher value-creation for labs, and better outcome for patients.
As of today, neither of these two scenarios is guaranteed – we still have time to shape this. To that end, I’ll humbly propose some thought frameworks, with great respect for the humanity of medicine’s most important discipline.
What problem should AI solve in pathology?
[They] were so preoccupied with whether or not they could, they didn’t stop to think if they should.
— Dr. Ian Malcolm, Jurassic Park
For roughly every dollar spent on actually caring for patients, hospitals spend nearly two on the system around it. Administrative expenditures are growing faster than direct patient care costs and now account for more than two-thirds of total hospital operating spend (3).
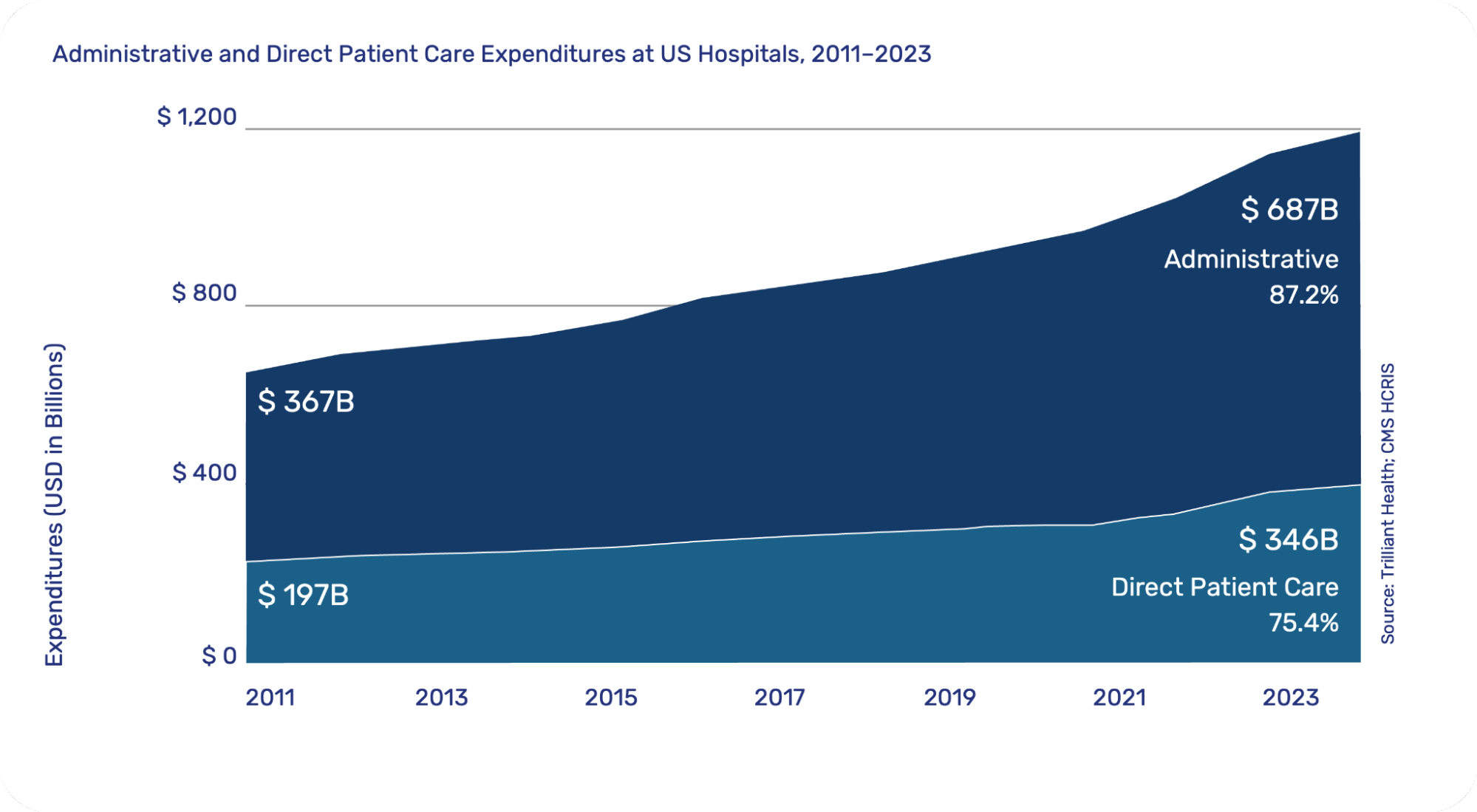
Source: Adapted from Trilliant Health; CMS HCRIS (2025)
Our healthcare system micromanages the experts it once revered. It extracts more time, piles on more documentation and clerical work, and protects against liability more than it protects its people and its patients.
We need to bend the right cost curve.
We know what this looks like in pathology. More than half of pathologists don’t have enough time to do their jobs well because of administrative burden (4). 85% of lab professionals report burnout tied to workload and operational pressure (5). All while Medicare reimbursements for anatomic pathology have declined over 30% in two decades (6).
The shape of the promised land
There are signs this can change. In clinical medicine, AI tools are already proving they can reduce administrative burden and elevate the practice of experts.
Abridge, an ambient AI platform, generates clinically useful (and billable) notes at the point of patient conversation. Ambient AI tools have reduced documentation time by 20%, cut after-hours charting by 30%, nearly halved the mental demand of note writing, and made 86% of primary care physicians more satisfied at work (7,8).
OpenEvidence has rapidly become a household name among physicians. The clinical evidence platform searches millions of peer-reviewed medical studies from trusted publications like NEJM and JAMA to help physicians provide the best care to patients. The product has reached the same number of active physicians in 11 months that similar traditional software took 11 years to reach (9).
Adoption isn’t being driven top-down by hospital IT departments. It’s growing from the ground up because these tools make the daily practice of medicine measurably better for stakeholders. Abridge and OpenEvidence users aren’t asking ‘why are you shoving another tool down my throat?’ They’re asking ‘what else can you build?’ Clinical experts are working at the top of their license, delivering human medicine.
These products are setting a blueprint for successful healthcare AI: bending the administrative cost curve, improving the work-life balance of practitioners, and aligning the economic incentives of patients, payers, providers, and product-builders.
What does this look like for pathology?
For pathologists, it’s reduced documentation burden, less after-hours work, better case context, less time commuting, and higher pay. For lab operations, it’s continuous quality, better efficiency, fewer tech integrations, and workloads for the staff they have (not the staff they wish they had). For lab leadership, it’s turning a cost center into a strategic asset, high-margin offerings, and a data-driven business.
We’ve gotten a glimpse already in pathology’s shift to digital. 10 years ago, when I first fell in love with pathology, most pathologists hated the idea of going digital. And for good reason: digital pathology products were terrible for pathologists – poor ergonomics, definitively slower than the microscope, developed by scanner or radiology companies, divorced from the complexities pathologists face, and unintegrated with the rest of the lab stack (some of these products are still on the market).
Many technology companies attempted to steamroll their way through this unsuccessfully. But product progress, combined with the cultural shakeup of COVID, has made digital the emerging standard. Newly minted pathologists want to work from home. Labs want to attract top talent and serve patient populations across wider geographies. Read efficiency on digital is outperforming the microscope.
Beyond this, though, pathology AI is synonymous with diagnostic AI: tumor detection, grading, scoring. These are incredibly promising tools, and they are already playing a critical role in advancing precision medicine. It’s certainly interesting technology to build, but they’re not the first thing pathologists and labs say they wish AI would solve. In some ways, they’ve distracted from the day-to-day tedium that is most ripe for offloading onto machines – context surfacing, clinical documentation, stain ordering, case routing, and prioritization, to name a few.
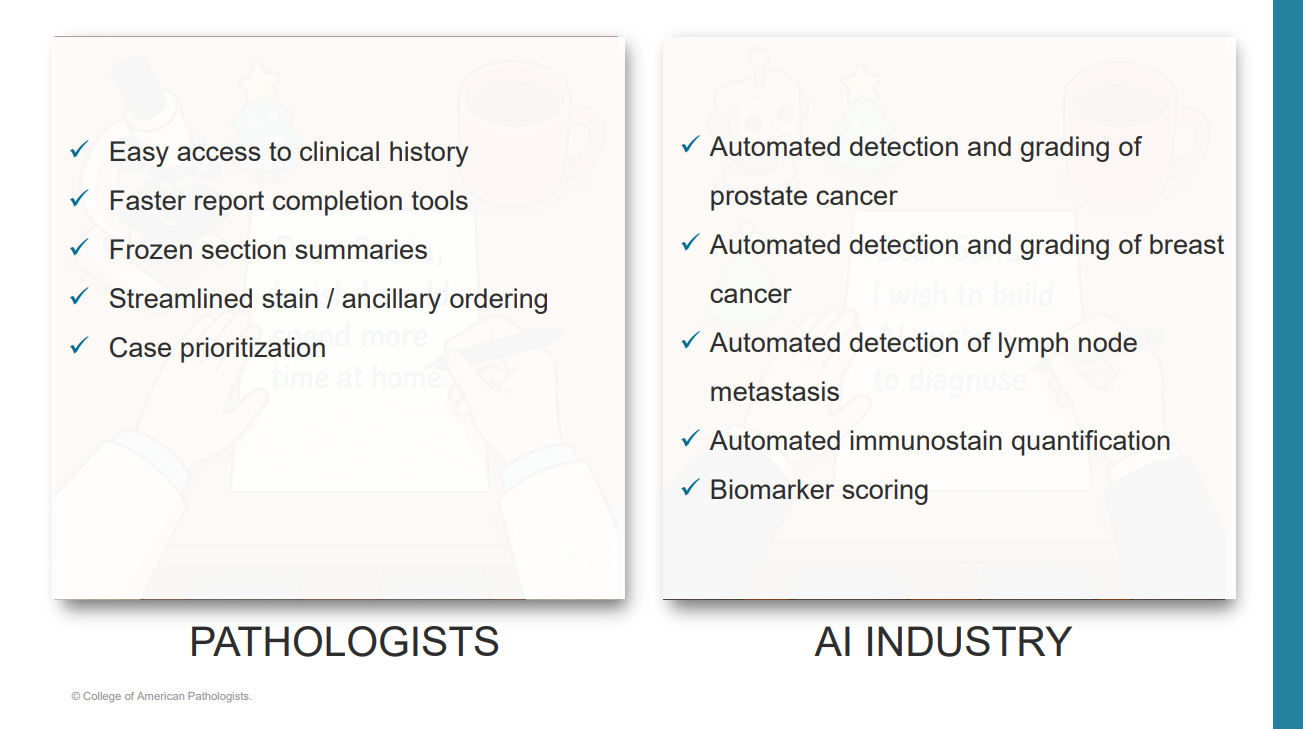
Source: Dibson Dibe Gondim, MD, FACP, CAP webinar (September 2025)
Non-diagnostic, or diagnostic-adjacent tasks, demand attention but not judgment. AI handles them without fatigue and without burning out. It removes the layer of drudgery and provides room to focus on what matters. I think this is under-discussed in the market, and newly addressable with LLMs and the agent layers built around them. Today’s models are certainly capable of handling this reliably, especially as increased digitization makes more context legible to the machine, but the hard work of integration, clinical validation, and enterprise integration is in the way of widespread adoption.
A world of infinite diagnostic demand
Clerical overhead and clinical context surfacing largely define the white space for AI in pathology as practiced today. But Jevons paradox is a “paradox” because it breaks one intuition for demand elasticity. In pathology, I think people struggle to imagine how much more diagnostic demand there could possibly be.
As models improve, pathology won’t just do its current job better. It will reach patients and power therapies that were previously too expensive or too complex to deploy. We’re already starting to use pathology in entirely new ways in clinical care because 1) complex therapies like ADCs require diagnostic solutions that didn’t previously exist, and 2) it’s cheaper to produce a diagnosis. AI is accelerating the speed with which new drugs are discovered, but their clinical success (in development and on market) is still dependent on the lab. Biomarker strategies that pharma shelved as impractical because they required expensive testing will suddenly become feasible and commercially viable.
And the ceiling keeps rising. Pathology is needed to get patients on the right therapy, match them to a clinical trial, or stratify patients by recurrence risk so oncologists can intervene before progression. In the limit, this looks like n-of-1 therapies, with highly personalized diagnostics for every patient. If not infinite diagnostic demand, multiple orders of magnitude more than today.

The window is open, but not for long.
I think this technology, as unsettling as it may be at first, can give that sense of purpose back. No doubt, greatly reshaping the discipline, but in the process, elevating the value of pathology, and shifting off the worst parts of being a pathologist and running a lab to the machine.
In other parts of medicine, clinicians are already saying that AI has changed how they feel about practicing. Because for the first time, technology actually made the day better.
I want pathologists to feel that too.
As Wharton professor Ethan Mollick said:
When a technology is this powerful and this unsettled, the choices that individuals and organizations make right now matter more.
The window to shape how AI changes pathology is open. But it will not stay open for long. I’m not waiting. I’ve been spending time with pathologists and lab leaders to talk about what AI means for the field and to help shape our AI products. If you want to be part of that conversation, follow me on LinkedIn or reach out directly.
Thank you to Dibson Dibe Gondim, Dr. Luis Cano, and Ethan Mollick for influencing this, directly or indirectly.
Sources
1. AI Index Steering Committee. Artificial Intelligence Index Report 2025. Stanford Institute for Human-Centered AI, Stanford University; April 2025. Accessed March 23, 2026. https://hai.stanford.edu/assets/files/hai_ai_index_report_2025.pdf
2. Owen D. AI in 2030: extrapolating current trends. Epoch AI; September 2025. Accessed March 23, 2026. https://epoch.ai/files/AI_2030.pdf
3. Oakes A. Hospital administrative expenditures exceed direct patient care by nearly 2x (data derived from CMS Healthcare Cost Report Information System [HCRIS], 2011–2023). Trilliant Health; October 17, 2025. Accessed March 23, 2026. https://www.trillianthealth.com/market-research/studies/hospital-administrative-expenditures-exceed-direct-patient-care-by-nearly-2x
4. Royal College of Pathologists. Workforce census 2025: morale and wellbeing of the pathology workforce. Royal College of Pathologists; August 11, 2025. Accessed March 23, 2026. https://www.rcpath.org/discover-pathology/news/workforce-census-2025-morale-and-wellbeing-of-the-pathology-workforce.html
5. Garcia E, Kundu I, Kelly M, Soles R, Mulder L, Talmon GA. The American Society for Clinical Pathology’s job satisfaction, well-being, and burnout survey of laboratory professionals. Am J Clin Pathol. 2020;153(4):470-486. doi:10.1093/ajcp/aqaa008
6. Miskiel S, Khreshi S, Khraishi R, Pagliaro A, Bombonati A. The decline of Medicare reimbursement in anatomic pathology. Am J Clin Pathol. 2024;162(suppl 1):S98. doi:10.1093/ajcp/aqae129.218
7. Duggan MJ, Dharwadkar P, Gur-Arie R, et al. Clinician experiences with ambient scribe technology to assist with documentation burden and efficiency. JAMA Netw Open. 2025;8(2):e2460637. doi:10.1001/jamanetworkopen.2024.60637
8. Stults CD, et al. Evaluation of an ambient artificial intelligence documentation platform for clinicians. JAMA Netw Open. 2025;8(5):e258614. doi:10.1001/jamanetworkopen.2025.8614
9. Contrary Research. 2026 Tech Trends Report. Contrary; 2026. Accessed March 23, 2026. https://research.contrary.com/tech-trends-report