Blog Post
How We Built Intelligence into the Pathology Platform
Coleman Stavish
16 Jul 2026

This post is about Concentriq AP and Concentriq LS, which are for Research Use Only, and the research and laboratory workflows they support. It does not describe diagnostic use. Concentriq AP-Dx, Proscia's product cleared for primary diagnosis, is a separate product and is not covered here.
We recently announced the Fifth Generation of Concentriq. This generation helps pathologists spend their time on high-judgment interpretation, and scientists move from an early signal to a confident program decision, faster. It does this by building clinically and scientifically grounded intelligence into the workflows experts already use across drug discovery, development, and case review.
Our announcement covered what we built and why we built it. This post is about the how.
We took a first-principles approach, working backwards from how pathologists and scientists actually operate. Years of learning from our customers showed us where workflow complexity slows them down, and where process competes with their judgment.
So we set a clear requirement: help experts spend less time on process and more time on the decisions that matter most. To meet this requirement, we needed to build a new platform architecture that makes intelligence native to Concentriq rather than bolted on top of it. The Fifth Generation brings domain-specific frontier models (vision, language, and multimodal) to the core of a technology stack built for enterprise-grade security, governance, and reliability.
This post walks through that architecture: the layers we built, how they fit together, and how they deliver novel functionality that labs and drug development programs can use today, while enabling scalable product growth as AI capabilities continue to improve. If what you read here resonates, come see the platform in action on July 28.
Why adding applications isn’t enough
Digitizing the practice of pathology through whole slide imaging is transformative in its own right, but many practitioners rightly understood it as just the first step in the evolution towards computational pathology. When tissue sections on glass slides are captured as whole slide images, new data are created. This new data can be used to train software algorithms and models capable of analyzing tissue. Model capabilities have improved as more image data has become available. Improved model capabilities enable software to provide more value to laboratories and drug development programs who have adopted whole slide imaging. This creates greater incentive for other organizations to adopt whole slide imaging. It’s been exciting to see this positive feedback loop repeat and accelerate over the past few years.
The algorithms and models most widely adopted to date have taken the form of task-specific applications. They have typically narrow inclusion criteria (e.g. a particular tissue and stain type) and produce an output relevant to a particular task being performed by a pathologist or scientist. Some such applications are FDA-cleared or -authorized to assist pathologists in specific diagnostic tasks. When many people encounter the term “pathology AI,” they think of this class of task-specific application.
Task- and image-specific applications have proven themselves to be useful in both research and clinical settings. Concentriq has executed hundreds of them across millions of images for our customers, and we intend for our platform to remain the best place for our customers to interact with these applications. But as my co-founder David wrote, these tools don’t address all of the problems and opportunities that our customers face.
A lot of the work that goes into keeping a lab running smoothly or advancing a research study involves more information than what is in a single image. Allocating for pathologists depends on the whole worklist and the clinical context behind each order. Stratifying patients in a drug development study depends on the full repository of cases and the molecular (and possibly outcome data) attached to them. Task- and image-specific AI applications don’t operate at that scope.
Some of what I'll describe throughout the rest of this post is running in 5.0, the first release of the Fifth Generation of Concentriq. Some is the foundation we've laid for what's coming next. The architecture is what makes it all possible.
Four layers, built around the decision
Concentriq is organized in four layers, from the data underneath to where a pathologist or scientist actually works.
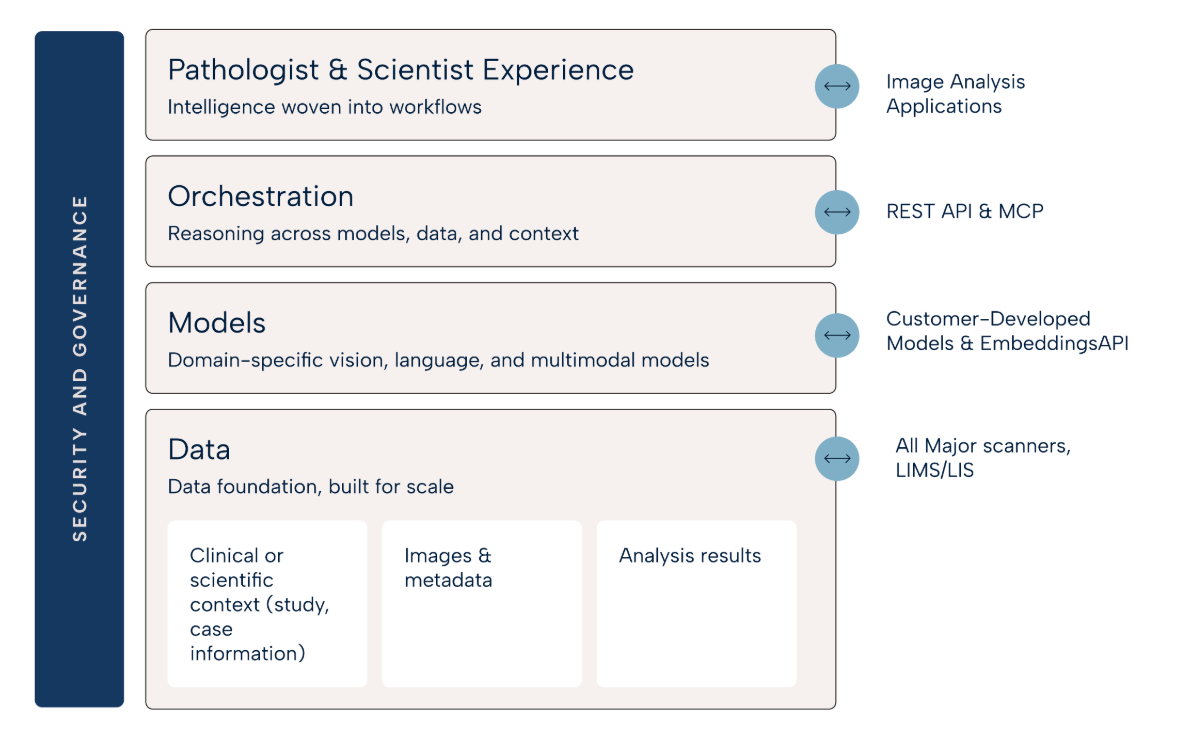
At the base is the data foundation. Its job is to join two kinds of data that usually sit apart: the whole slide images, and the patient, study, and case information from the LIS. Concentriq pairs each image with the metadata the lab holds about it, the specimen, stain, procedure, and the rest of the case, so the image carries that context wherever it goes.
A case is the connected set of images and information that belong to it: slide-level morphology, patient history, lab-specific protocols, translational data, and the results of every analysis run against them. That context is the basis for everything above it. Whether a model, an agent, or a person is reasoning about the case, they start from the same place.
Above the data are the models. Reading a whole slide image well takes models built for pathology. General-purpose encoders don't transfer well to tissue: self-supervised models pretrained on large collections of pathology slides outperform encoders carried over from general-purpose datasets across a wide range of tasks1. We use pathology-specific models and treat their embeddings as a shared representation that many tasks can draw on, so we aren't training a separate model for every task.
This is also where models run. Pathology images are large; a routine clinical slide runs from a few hundred megabytes to a few gigabytes. Fluorescence images for specialty work can be ten times larger, and multiplexed fluorescence images for research a hundred times larger. Moving images of that size to wherever a model happens to run is costly, so Concentriq Compute executes models as containerized workloads on elastic infrastructure, beside the data. Images don’t have to leave the platform, and deploying the next model requires a container and a configuration file rather than a new infrastructure project. Built-in models, customer-developed models, and vendor-developed models can run on this same infrastructure.
Then comes orchestration. This layer decides what happens next, and what the expert sees, by drawing on everything beneath it: the images, their metadata, and the models. Because every image arrives already joined to its case, the platform knows what kind of case and image are in front of the expert, and adapts to both.
Features activate on that basis, with the tools and overlays that fit a given specimen or stain coming up when they're relevant. Analyses behave the same way, with specific tasks running automatically on the image and case types they're meant for. The layer can also carry context across a case or study, such as a relevant prior, what's already in the report, where the case sits in the workflow. It can use that to prioritize, route, and prepare the work. Standalone applications are usually unable to achieve this.
At the top is where the people of pathology work. We put significant effort into observing how users work, digitally and non-digitally, and building a product experience intended to feel natural to pathologists. Dr. Daniel Roberts, the medical director of digital pathology at Cleveland Clinic, described it this way: "They took the muscle memory our pathologists have built over decades at the microscope and made it native to the digital screen. No one else has done that." That's the standard we work to.
This shapes how we build, too. Our AI scientists, designers, and engineers work alongside pathologists, clinicians, and R&D scientists the whole way, not just at sign-off. You can't guess your way to software that fits how an expert thinks. The best feedback we get comes from real usage at scale, across tens of thousands of pathologists and scientists.
Open at every layer
Intelligence built into the platform is still open at every layer. We provide a great deal of it, and our customers and partners extend the rest.
Openness starts at the data layer: all of your data comes in, and it keeps coming in as your organization grows. For labs, every acquisition or expansion brings another site running a different technology stack, with its own scanners, formats, and systems. CROs and biopharma teams run many studies at once, from exploratory next-gen science to tightly controlled trial protocols, each with its own scanners, assays, formats, and requirements.
That’s why Concentriq supports the vast majority of scanners and every major image format, DICOM included, as well as bi-directional integrations with the top LIS and LIMS vendors. So what you run today keeps working, and what you bring on tomorrow does, too.
At the model layer, you can use the models we provide or bring your own, and interact with them through our Embeddings API to build your own pipelines. Third-party and customer-built tools integrate through the Image Analysis Service, our integration interface. An application registers with the service, (optionally) runs on Concentriq Compute, and posts results back as overlays, heatmaps, and structured values that render in the viewer, each linked to the source image and run that produced it. Because that path is standardized, adding a tool is straightforward. As a proof of concept, our internal team took QuPath, one of the most widely used open-source pathology tools, and had it running on the platform in a matter of days.
At the orchestration layer, the platform is open to agents. Every Concentriq service is exposed through a REST API that customers, and the agents they build, can call directly. Because those APIs are complete and open, reaching Concentriq through the Model Context Protocol, the open standard for connecting agents to tools and data2, becomes feasible.
Open interfaces matter because a closed platform caps what its customers can build. We want our customers, and the tools they choose, to extend the platform directly.
One foundation, from discovery to case review
The implications for clinical and scientific work are significant on their own. But the even bigger opportunity comes from connecting them.
Historically, the work of discovering a biomarker and the work of deploying it in practice have lived in separate worlds. Research teams worked with one set of data, tools, and workflows. Clinical teams worked with another. The result has been a long and often fragmented path from biological insight to clinically useful assay.
Concentriq’s architecture can shorten that distance. Millions of cases are reviewed on Concentriq each year, creating real-world data that brings images together with structured reports, and in some cases, molecular results and outcomes. This is exactly what biopharma needs to discover biomarkers, design trials, and develop companion diagnostics.
Just as important, the same foundation can support the path back to the clinic. A biomarker identified in research can move more naturally toward validation, deployment, and use in the clinic because the underlying data, models, workflows are no longer disconnected from the clinical infrastructure in which they ultimately need to operate.
My co-founder David also recently wrote about the coming rise in testing demand in the age of AI, as biomarker strategies that were once too expensive or impractical to run become feasible. In that world, the organizations that can connect discovery and clinical testing through one platform will be better positioned to capture this value and help get the right therapy to the right patient faster.
Trust is part of the architecture
In pathology, software has to earn trust before it's used at all. We work under the same constraints as the labs we serve: reliability, clinical validation, reproducibility, auditability, and regulated change control. We build for those constraints directly.
We classify and validate changes according to their risk. We keep a clear record of how each result was produced.
Because intelligence is built into an enterprise-grade platform, it inherits the same security, access, and data-protection controls Concentriq already operates under. This means that your data stays yours, your data stays protected, and the AI runs inside the same independently audited security program as the rest of the platform, not in a separate system with its own rules.
Because the controls are part of the architecture, we can move quickly to bring more value to our customers, and still stand behind every result. Building governance into the platform lets our customers adopt the latest AI advancements sooner, and do it without putting compliance at risk.
Why now and what’s next
Demand for what pathology can tell us is rising, and it will keep rising as targeted therapies and companion diagnostics multiply. The various technology components and regulatory frameworks required to meet that demand finally exist. Whole slide imaging is now well established. Models built specifically for pathology have matured. Clinical-grade agents and early AI-driven companion diagnostics are arriving now. For the first time, every layer needed to build intelligence into the platform is available at once.
That's what we've spent the last few quarters building. The Fifth Generation architecture starts from one position: pathology intelligence belongs inside the platform, not outside it. One foundation carries the data, models, and orchestration; the interfaces stay open at every layer; context follows the case; and the pathologist or scientist stays in control of the intelligence. It's the right foundation for where pathology is going.
On July 28, we’ll dive deep into how the Fifth Generation of Concentriq works, alongside the pathologists and scientists who helped shape it. We hope you’ll join us.
---
1 For example, Chen RJ, Ding T, Lu MY, et al. Towards a general-purpose foundation model for computational pathology. Nat Med. 2024;30(3):850-862. This self-supervised model was pretrained on more than 100 million images from over 100,000 H&E whole-slide images (more than 77 TB) across 20 tissue types and evaluated on 34 tasks, outperforming encoders transferred from general-purpose image datasets. See also: Lu MY, Chen B, Williamson DFK, et al. A visual-language foundation model for computational pathology. Nat Med. 2024;30(3):863-874; and Xu H, Usuyama N, Bagga J, et al. A whole-slide foundation model for digital pathology from real-world data. Nat Med. 2024.
2 The Model Context Protocol, an open standard introduced by Anthropic in November 2024 and since adopted across the industry, standardizes how AI agents connect to external tools and data sources.